


 Sign Out
Sign Out



Pharmacology: Pharmacodynamics: Mode of action: Tiotropium, a long acting muscarinic antagonist and olodaterol a long acting beta2-adrenergic are administered together in the SPIOLTO RESPIMAT soft mist inhaler. These two active ingredients provide additive bronchodilation due to their different mode of action and different locations of the target receptors in the airways.
Tiotropium: Tiotropium bromide is a long-acting, muscarinic receptor antagonist (LAMA), in clinical medicine often called an anticholinergic. It has a similar affinity to the subtypes of muscarinic receptors M1 to M5. In the airways, inhibition of M3-receptors at the smooth muscle results in relaxation. The competitive and reversible nature of antagonism was shown with human and animal origin receptors and isolated organ preparations. In pre-clinical in vitro as well as in vivo studies bronchoprotective effects were dose-dependent and lasted longer than 24 hours. The long duration of the effect is likely to be due to its very slow dissociation from M3-receptors, exhibiting a significantly longer dissociation half-life than that seen with ipratropium. As an N-quaternary anticholinergic tiotropium is topically (broncho-) selective when administered by inhalation, demonstrating an acceptable therapeutic range before giving rise to systemic anti-cholinergic effects.
Dissociation from M2-receptors is faster than from M3, which in functional in vitro studies, elicited (kinetically controlled) receptor subtype selectivity of M3 over M2.
The high potency and slow receptor dissociation found its clinical correlate in significant and long-acting bronchodilation in patients with COPD.
The bronchodilation following inhalation of tiotropium is primarily a local effect (on the airways) not a systemic one.
Olodaterol: Olodaterol has a high affinity and high selectivity to the human beta2-adrenoceptor. In vitro studies have shown that olodaterol has 241-fold greater agonist activity at beta2- adrenoceptors compared to beta1-adrenoceptors and 2299-fold greater agonist activity compared to beta3-adrenoceptors. The compound exerts its pharmacological effects by binding and activation of beta2-adrenoceptors after topical administration by inhalation.
Activation of these receptors in the airways results in a stimulation of intracellular adenyl cyclase, an enzyme that mediates the synthesis of cyclic-3',5' adenosine monophosphate (cAMP). Elevated levels of cAMP induce bronchodilation by relaxation of airway smooth muscle cells.
Olodaterol has the pre-clinical profile of a long-acting selective beta2-adrenoceptor agonist (LABA) with a fast onset of action and duration of action of at least 24 hours.
Beta-adrenoceptors are divided into three subtypes, beta1-adrenoceptors predominantly expressed on cardiac muscle, beta2-adrenoceptors predominantly expressed on airway smooth muscle and beta3-adrenoceptors predominantly expressed on adipose tissue. Beta2-agonists cause bronchodilation. Although the beta2-adrenoceptor is the predominant adrenergic receptor in the airway smooth muscle it is also present on the surface of a variety of other cells, including lung epithelial and endothelial cells and in the heart. The precise function of beta2-receptors in the heart is not known, but their presence raises the possibility that even highly selective beta2-adrenergic agonists may have cardiac effects.
Clinical Trials: Effects on cardiac electrophysiology: Tiotropium: In a dedicated QT study involving 53 healthy volunteers, tiotropium inhalation powder 18 microgram and 54 microgram (i.e. three times the therapeutic dose) over 12 days did not significantly prolong QT intervals of the ECG.
Olodaterol: The effect of olodaterol on the QT/QTc interval of the ECG was investigated in 24 healthy male and female volunteers in a double-blind, randomised, placebo- and active (moxifloxacin) controlled study. Olodaterol at single doses of 10, 20, 30 and 50 microgram, demonstrated that compared with placebo, the mean changes from baseline in QT interval over 20 minutes to 2 hours after dosing increased dose-dependently from 1.6 (10 microgram olodaterol) to 6.5 ms (50 microgram olodaterol), with the upper limit of the two-sided 90% confidence intervals being less than 10 ms at all dose levels.
The effect of 5 microgram and 10 microgram olodaterol on heart rate and rhythm was assessed using continuous 24-hour ECG recording (Holter monitoring) in a subset of 772 patients in the 48-week, placebo-controlled Phase 3 Trials. There were no dose- or time-related trends or patterns observed for the magnitudes of mean changes in heart rate or premature beats. Shifts from baseline to the end of treatment in premature beats did not indicate meaningful differences between olodaterol 5 microgram, 10 microgram and placebo.
SPIOLTO RESPIMAT: In two 52-week randomized, double-blind trials using SPIOLTO RESPIMAT that enrolled 5162 patients with COPD, ECG assessments were performed post-dose on days 1, 85, 169, and 365. In a pooled analysis the number of subjects with changes from baseline-corrected QT interval of >30 msec using both the Bazett (QTcB) and Fredericia (QTcF), corrections of QT for heart rate ranged from 4.9-6.4% (QTcB) and 1.3-4.7% (QTcF) for the SPIOLTO RESPIMAT group compared to 5.0-6.0% (QTcB) and 1.3-4.4% (QTcF) for olodaterol 5 microgram and 5.3-6.5% (QTcB) and 2.1-4.6% (QTcF) for tiotropium 5 microgram across the assessments conducted.
Clinical efficacy and safety: The Phase III clinical development program for SPIOLTO RESPIMAT included three randomised, double-blind trials: (i) two replicate, 52 week parallel group trials comparing SPIOLTO RESPIMAT with tiotropium 5 microgram and olodaterol 5 microgram (1029 received SPIOLTO RESPIMAT) [Trials 1 and 2]; (ii) one 6 week cross-over trial comparing SPIOLTO RESPIMAT with tiotropium 5 microgram and olodaterol 5 microgram and placebo (139 received SPIOLTO RESPIMAT) [Trial 3].
In these trials, the comparator products, tiotropium 5 microgram, olodaterol 5 microgram and placebo, were administered via the RESPIMAT inhaler.
All studies included lung function measurements (forced expiratory volume in one second, FEV1). In the 52 week studies, lung function was measured up to 3 hrs post-dose (12 hrs post- dose in a sub-set of patients) and at 23-24 hrs post-dose; the primary lung function efficacy endpoints were change from pre-treatment baseline (response) in FEV1 AUC0-3h and trough FEV1 after 24 weeks. In the 6 week study, lung function was measured up to 12 hrs post-dose and at 22-24 hrs post-dose; the primary efficacy endpoint was FEV1 AUC0-24h response after 6 weeks. The 52 week trials also included the St. George's Respiratory Questionnaire (SGRQ) as a primary endpoint as a measure of health-related quality of life and the Mahler Transition Dyspnoea Index (TDI) as a key secondary endpoint as a measure of dyspnoea.
Patients enrolled into the Phase III program were 40 years of age or older with a clinical diagnosis of COPD, had a smoking history of more than 10 pack years and had moderate to very severe pulmonary impairment (post-bronchodilator FEV1 less than 80% predicted normal (GOLD Stage 2-4); post-bronchodilator FEV1 to FVC ratio of less than 70%).
Patient characteristics: The majority of the 5162 patients recruited in the global, 52 week trials [Trials 1 and 2] were male (73%), white (71%) or Asian (25%), with a mean age of 64.0 years. Mean post-bronchodilator FEV1 was 1.37 L (GOLD 2 [50%], GOLD 3 [39%], and GOLD 4 [11%]). Mean β2-agonist responsiveness was 16.6% of baseline (0.171 L). Pulmonary medications allowed as concomitant therapy included inhaled steroids [47%] and xanthine's [10%].
The 6 week trial [Trial 3] was conducted in Europe and North America. The majority of the 219 recruited patients were male (59%) and white (99%), with a mean age of 61.1 years. Mean post-bronchodilator FEV1 was 1.55 L (GOLD 2 [64%], GOLD 3 [34%], GOLD 4 [2%]). Mean β2-agonist responsiveness was 15.9% of baseline (0.193 L). Pulmonary medications allowed as concomitant therapy included inhaled steroids [41%] and xanthines [4%].
Lung function: In the 52 week trials, SPIOLTO RESPIMAT, administered once daily in the morning, provided clear improvement in lung function within 5 minutes after the first dose compared to tiotropium 5 microgram (mean increase in FEV1 of 0.137 L for SPIOLTO RESPIMAT vs. 0.058 L for tiotropium 5 microgram [p<0.0001] and 0.125 L for olodaterol 5 microgram [p=0.16]). In both studies, significant improvements were observed in FEV1 AUC0-3h response and trough FEV1 response after 24 weeks (lung function primary endpoints) for SPIOLTO RESPIMAT compared to tiotropium 5 microgram and olodaterol 5 microgram (see Table 1).
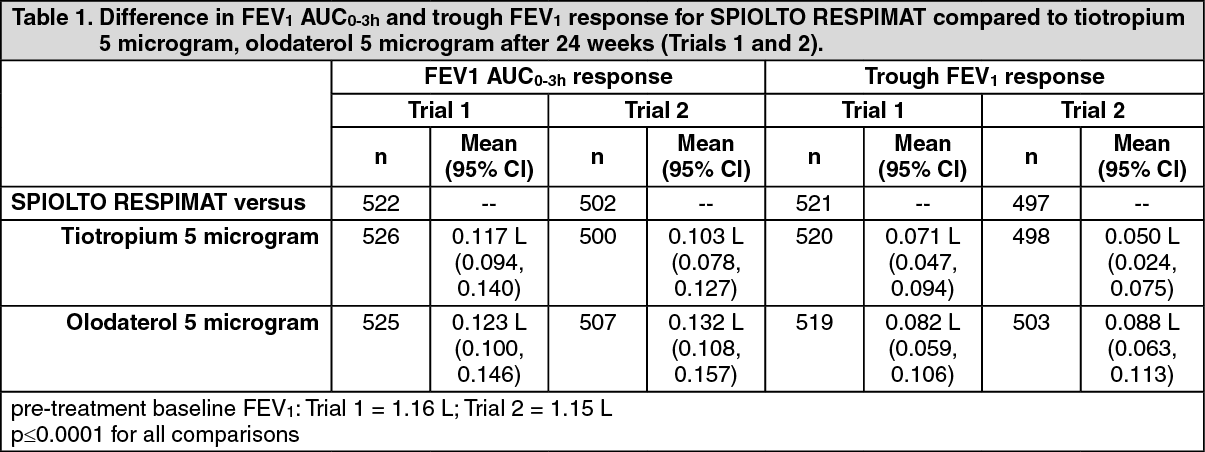 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe increased bronchodilator effects of SPIOLTO RESPIMAT compared to tiotropium 5 microgram and olodaterol 5 microgram were maintained throughout the 52 week treatment period. SPIOLTO RESPIMAT also improved morning and evening PEFR (peak expiratory flow rate) compared to tiotropium 5 microgram and olodaterol 5 microgram as measured by patient's daily recordings.
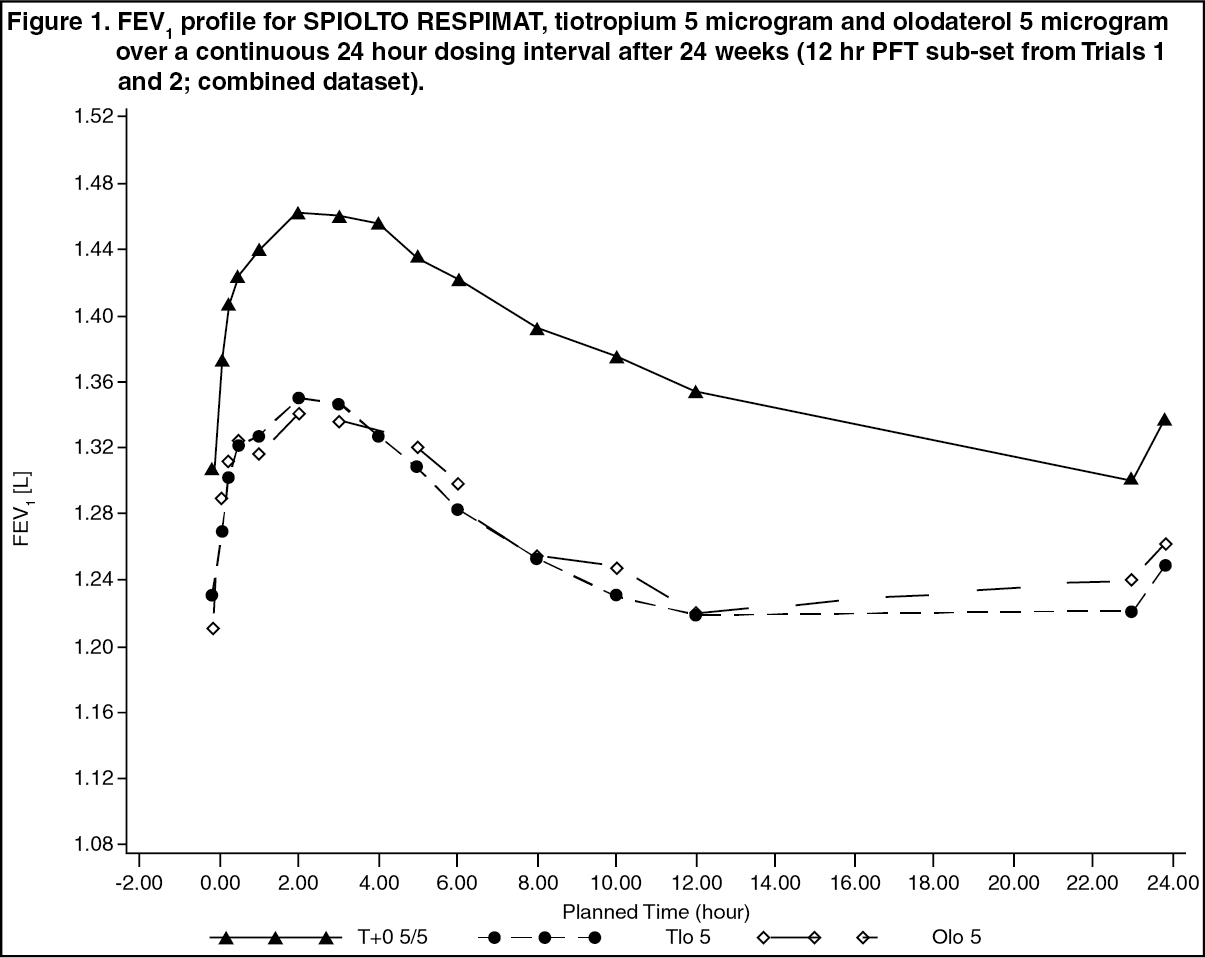
In the sub-set of patients who completed extended lung function measurements up to 12 hrs post-dose, SPIOLTO RESPIMAT showed a significantly greater FEV1 response compared to tiotropium 5 microgram and olodaterol 5 microgram over the full 24 hour dosing interval (see Figure 1 and Table 2).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image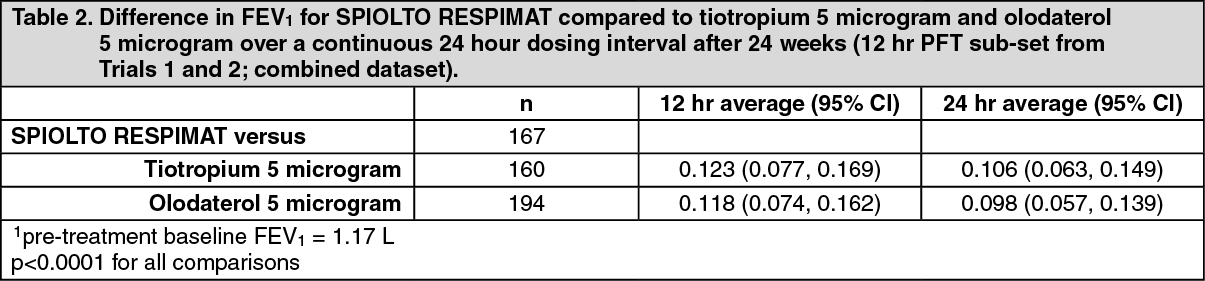 Click on icon to see table/diagram/image
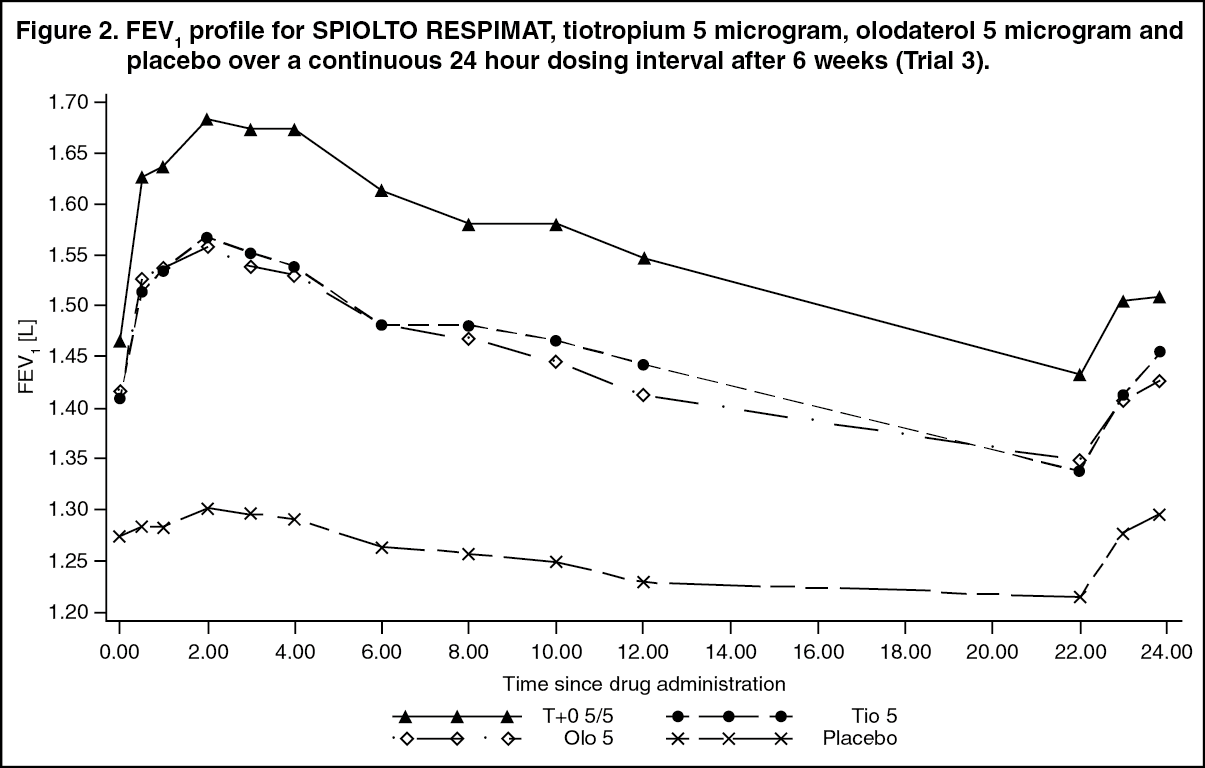
Click on icon to see table/diagram/imageIn the 6 week trial, SPIOLTO RESPIMAT showed a significantly greater FEV1 response compared to tiotropium 5 microgram, olodaterol 5 microgram and placebo over the full 24 hour dosing interval (see Figure 2 and Table 3).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
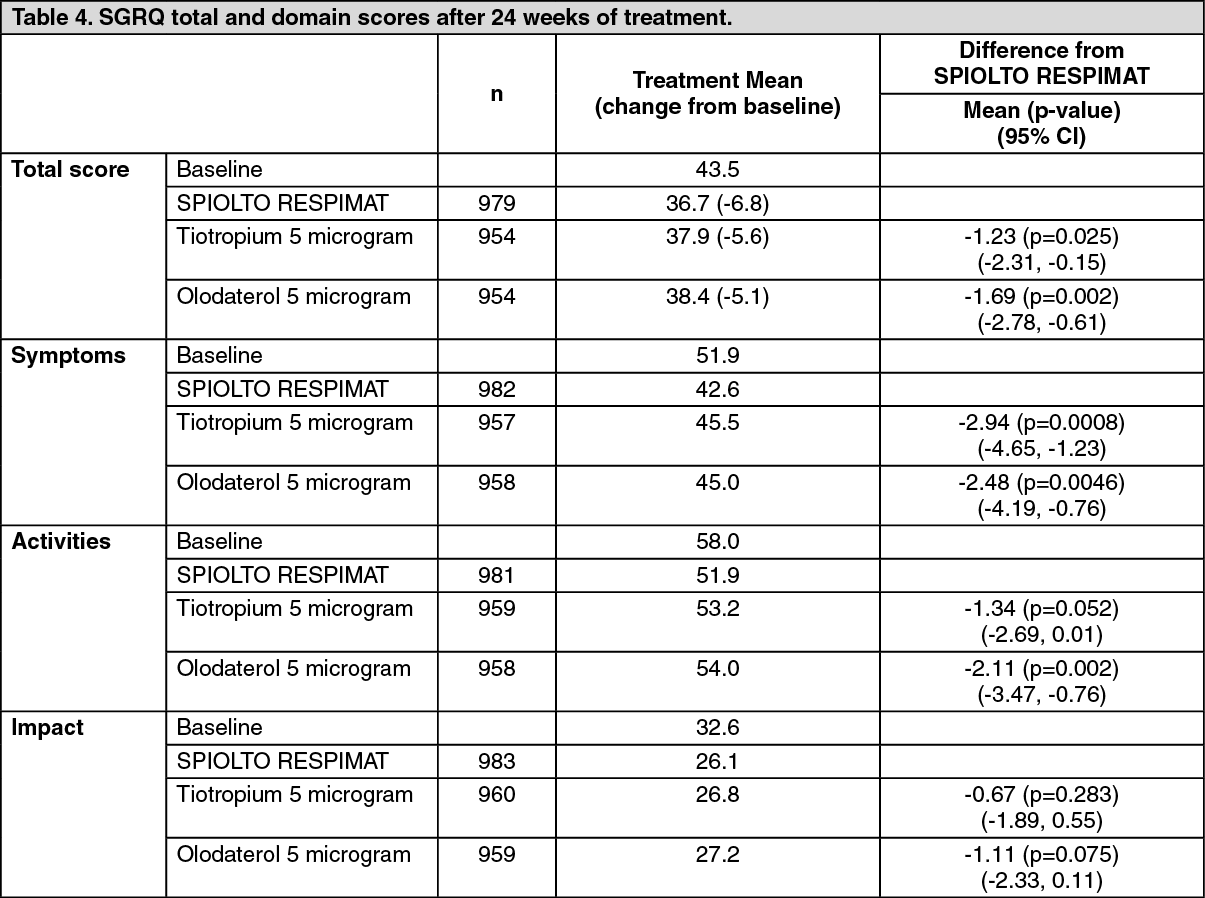
Click on icon to see table/diagram/imageHealth-related Quality of Life: After 24 weeks, SPIOLTO RESPIMAT significantly improved mean SGRQ total score compared to tiotropium 5 microgram and olodaterol 5 microgram (Table 4); improvements were seen in all SGRQ domains. More patients treated with SPIOLTO RESPIMAT had a clinically meaningful improvement in SGRQ total score (MCID, defined as a decrease of at least 4 units from baseline) compared to tiotropium 5 microgram (57.5% vs. 48.7%, p=0.0001) and olodaterol 5 microgram (57.5% vs. 44.8%, p<0.0001). (See Table 4).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn two additional 12-week, placebo-controlled clinical trials, SGRQ total score at 12 weeks was also included as primary endpoint as a measure of healthy-related quality of life.
In the 12-week trials, SPIOLTO RESPIMAT demonstrated an improvement compared with placebo at week 12 in mean SGRQ total score (primary endpoint) of -4.9 (95% CI: -6.9, -2.9; p<0.0001) and -4.6 (95% CI: -6.5, -2.6; p<0.0001). In a pooled analysis of the 12-week trials, the proportion of patients with a clinically meaningful decrease in SGRQ total score (defined as a decrease of at least 4 units from baseline) at week 12 was greater for SPIOLTO RESPIMAT (52%) compared with tiotropium 5 microgram (41%; odds ratio: 1.56 (95% CI: 1.17, 2.07), p=0.0022) and placebo (32%; odds ratio: 2.35 (95% CI: 1.75, 3.16), p <0.0001).
Dyspnoea: After 24 weeks, SPIOLTO RESPIMAT significantly improved mean TDI focal score compared to tiotropium 5 microgram and olodaterol 5 microgram (Table 5). More patients treated with SPIOLTO RESPIMAT had a clinically meaningful improvement in TDI focal score (MCID, defined as a value of at least 1 unit) compared to tiotropium 5 microgram (54.9% vs. 50.6%, p=0.0546) and olodaterol 5 microgram (54.9% vs. 48.2%, p=0.0026). (See Table 5).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageRescue Medication Use: Patients treated with SPIOLTO RESPIMAT used less daytime and night-time rescue salbutamol compared to patients treated with tiotropium 5 microgram and olodaterol 5 microgram.
Patient Global Rating: Patients treated with SPIOLTO RESPIMAT perceived a greater improvement in their respiratory condition compared to tiotropium 5 microgram and olodaterol 5 microgram, as measured by a Patient's Global Rating (PGR) scale.
Exacerbations: Tiotropium 5 microgram has previously demonstrated a statistically significant reduction in risk of a COPD exacerbation compared to placebo. COPD exacerbations was included as an additional endpoint in the 52 week pivotal trials (Trials 1 and 2). In the combined dataset, the proportion of patients experiencing a moderate/severe COPD exacerbation was 27.7% for SPIOLTO RESPIMAT and 28.8% for tiotropium 5 microgram (p=0.39). These studies were not specifically designed to evaluate the effect of treatments on COPD exacerbations.
Inspiratory capacity, breathing discomfort and exercise endurance: The effect of SPIOLTO RESPIMAT on inspiratory capacity, breathing discomfort and symptom-limited exercise endurance was investigated in three randomised, double-blind trials in COPD patients: (i) two replicate, 6 week cross-over trials comparing SPIOLTO RESPIMAT with tiotropium 5 microgram, olodaterol 5 microgram and placebo during constant work rate cycling (450 received SPIOLTO RESPIMAT) [Trials 4 and 5]; (ii) one 12 week parallel group trial comparing SPIOLTO RESPIMAT with placebo during constant work rate cycling (139 received SPIOLTO RESPIMAT) and constant speed walking (sub-set of patients) [Trial 6].
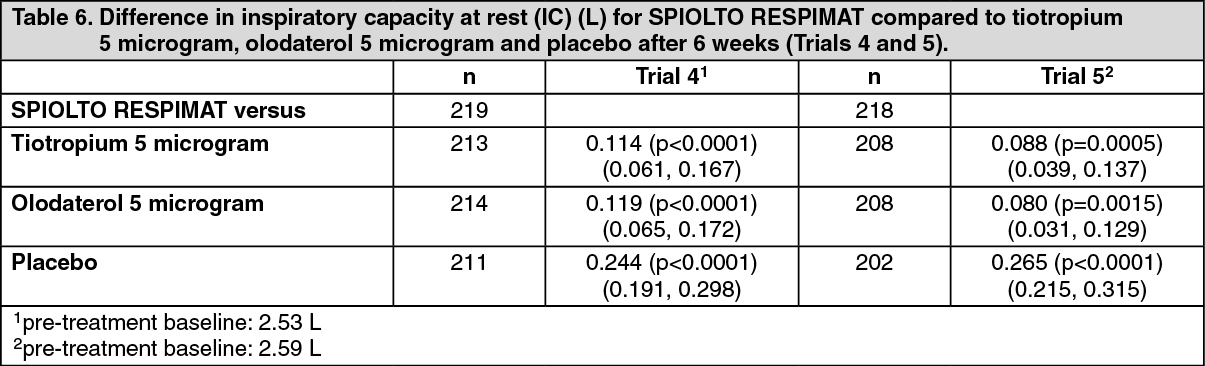
SPIOLTO RESPIMAT significantly improved inspiratory capacity compared to tiotropium 5 microgram, olodaterol 5 microgram and placebo after 6 weeks (Trials 4 and 5; Table 6) and compared to placebo after 12 weeks (0.234 L, p<0.0001; 95% CI: 0.133, 0.336; Trial 6). (See Table 6).
 Click on icon to see table/diagram/image
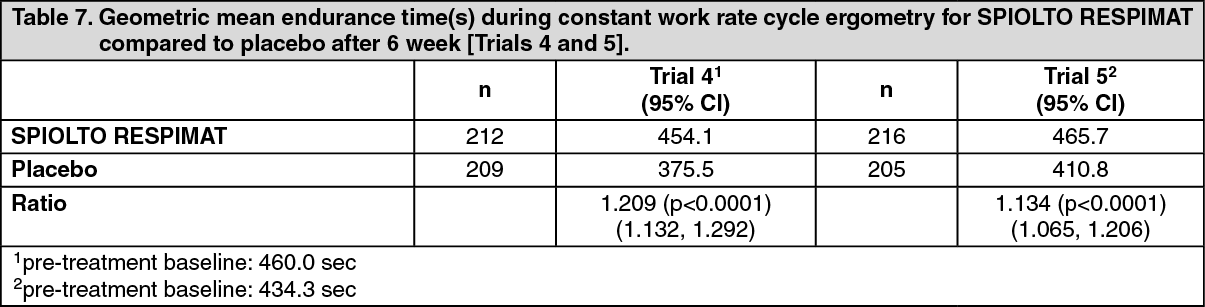
Click on icon to see table/diagram/imageIn Trials 4 and 5, SPIOLTO RESPIMAT improved endurance time during constant work rate cycling by 20.9% and 13.4% compared to placebo (Table 7). In Trial 6, SPIOLTO RESPIMAT improved endurance time during constant work rate cycling by 12.6% after the first dose (in a sub-set of patients), by 22.9% after 6 weeks and by 13.8% after 12 weeks compared to placebo. The endurance time during constant speed walking (in a sub-set of patients) increased by 20.6% after 6 weeks and by 20.9% after 12 weeks compared to placebo although the result was not statistically significant (Table 8).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image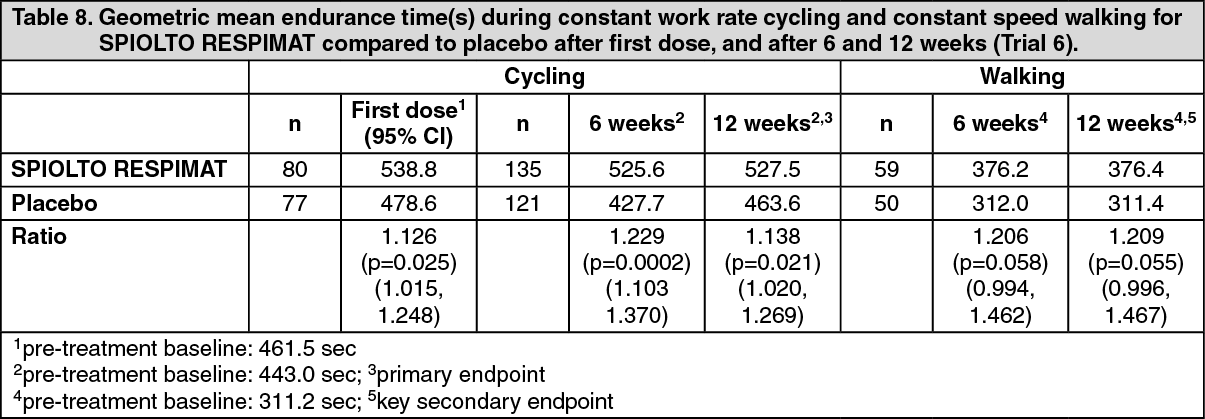 Click on icon to see table/diagram/image
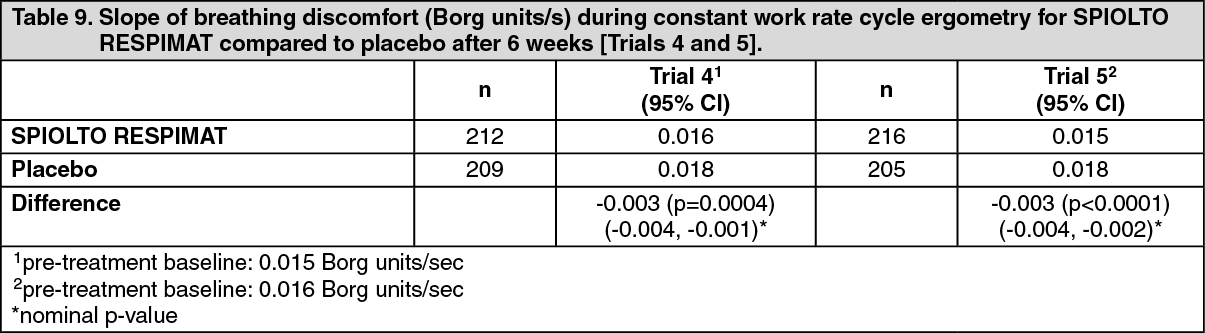
Click on icon to see table/diagram/imageIn Trials 4 and 5, SPIOLTO RESPIMAT decreased the slope of breathing discomfort during constant work rate cycling compared to placebo (nominal p<0.0005; Table 9). (See Table 9).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacokinetics: When tiotropium and olodaterol were administered in combination by the inhaled route, the pharmacokinetic parameters for each component were similar to those observed when each active substance was administered separately.
Tiotropium and olodaterol demonstrate linear pharmacokinetics in the therapeutic range. On repeated once-daily inhalation administration, steady state of tiotropium is reached by day 7. Steady state of olodaterol is achieved after 8 days of once-daily inhalation, and accumulation is up to 1.8-fold as compared to a single dose.
Absorption: Tiotropium: Urinary excretion data from young healthy volunteers suggests that approximately 33% of the dose inhaled via the RESPIMAT inhaler reaches the systemic circulation. The absolute bioavailability from an orally administered solution was found to be 2-3%. Maximum tiotropium plasma concentrations are observed 5-7 minutes after the inhalation via RESPIMAT.
Olodaterol: In healthy volunteers the absolute bioavailability of olodaterol following inhalation was estimated to be approximately 30%, whereas the absolute bioavailability was below 1% when given as an oral solution. Maximum olodaterol plasma concentrations generally are reached within 10 to 20 minutes following drug inhalation via RESPIMAT.
Distribution: Tiotropium has a plasma protein binding of 72% and shows a volume of distribution of 32 L/kg. Studies in rats have shown that tiotropium does not penetrate the blood-brain barrier to any relevant extent.
Olodaterol has a plasma protein binding of approximately 60% and shows a volume of distribution of 1110 L.
Biotransformation: Tiotropium: The extent of metabolism is small. This is evident from 74% of an intravenous dose being excreted in the urine as unchanged drug. The ester tiotropium is nonenzymatically cleaved into its alcohol and acid component (N-methylscopine and dithienylglycolic acid, respectively), both not binding to muscarinic receptors. In vitro experiments with human liver microsomes and human hepatocytes suggest that some further drug (<20% of the dose after intravenous administration) is metabolized by cytochrome P450 (CYP) 2D6 and 3A4 dependent oxidation and subsequent glutathione conjugation to a variety of Phase II-metabolites.
Olodaterol is substantially metabolized by direct glucuronidation and by O-demethylation at the methoxy moiety followed by conjugation. Of the six metabolites identified, only the unconjugated demethylation product (SOM 1522) binds to β2-receptors; this metabolite however is not detectable in plasma after chronic inhalation of the recommended therapeutic dose or doses of up to 4-fold higher. Cytochrome P450 isozymes CYP2C9 and CYP2C8, with negligible contribution of CYP3A4, are involved in the O-demethylation of olodaterol, while uridine diphosphate glycosyl transferase isoforms UGT2B7, UGT1A1, 1A7 and 1A9 were shown to be involved in the formation of olodaterol glucuronides.
Elimination: Tiotropium: Intravenously administered tiotropium is mainly excreted unchanged in urine (74%). The total clearance in healthy volunteers is 880 mL/min. After inhalation by COPD patients to steady-state, urinary excretion is 18.6% of the dose, the remainder being mainly non-absorbed drug in gut that is eliminated via the faeces. The renal clearance of tiotropium exceeds the glomerular filtration rate, indicating active secretion into the urine. The effective half-life of tiotropium following inhalation by COPD patients ranges between 27 and 45 h.
Olodaterol: Total clearance of olodaterol in healthy volunteers is 872 mL/min, and renal clearance is 173 mL/min. The terminal half-life following intravenous administration is 22 hrs. The terminal half-life following inhalation in contrast is about 45 hrs, indicating that the latter is determined by absorption rather than by elimination processes.
Following intravenous administration of [14C]-labelled olodaterol, 38% of the radioactive dose was recovered in the urine and 53% was recovered in feces. The amount of unchanged olodaterol recovered in the urine after intravenous administration was 19%. Following oral administration, only 9% of the radioactivity was recovered in urine, while the major portion was recovered in feces (84%). More than 90% of the dose was excreted within 6 and 5 days following intravenous and oral administration, respectively. Following inhalation, excretion of unchanged olodaterol in urine within the dosing interval in healthy volunteers at steady state accounted for 5-7% of the dose.
Characteristics in Patients: Tiotropium: As expected for all predominantly renally excreted drugs, advancing age was associated with a decrease of tiotropium renal clearance from 347 mL/min in COPD patients <65 years to 275 mL/min in COPD patients ≥65 years. This did not result in a corresponding increase in AUC0-6,ss or Cmax,ss values.
Olodaterol: A pharmacokinetic meta-analysis utilizing data from 2 controlled clinical trials that included 405 patients with COPD and 296 patients with asthma showed that no dose adjustment is necessary due to effects of age, gender and weight on systemic exposure to olodaterol.
Comparison of pharmacokinetic data within and across studies with olodaterol revealed a trend for higher systemic exposure in Japanese and other Asians than in Caucasians.
No safety concerns were identified in clinical studies with olodaterol in Caucasians and Asians of up to one year with olodaterol doses up to twice the recommended therapeutic dose.
Renal Insufficiency: Tiotropium: Following once daily inhaled administration of tiotropium to steady-state in COPD patients with mild renal impairment (CLCR 50-80 mL/min) resulted in slightly higher AUC0-6,ss (between 1.8 to 30% higher) and similar Cmax,ss compared to patients with normal renal function (CLcr >80 mL/min). In subjects with moderate to severe renal impairment (CLCR <50 ml/min) intravenous administration of tiotropium resulted in twofold higher total exposure (82% higher AUC0-4h and 52% higher Cmax) compared to subjects with normal renal function, which was confirmed by observations after dry powder inhalation.
Olodaterol: In subjects with severe renal impairment (CLCR <30 mL/min) systemic exposure to olodaterol was on average 1.4-fold increased. This magnitude of exposure increase does not raise any safety concerns given the safety experience of treatment with olodaterol in clinical studies of up to one year at doses up to twice the recommended therapeutic dose.
Hepatic Insufficiency: Tiotropium: Liver insufficiency is not expected to have any relevant influence on tiotropium pharmacokinetics. Tiotropium is predominantly cleared by renal elimination (74% in young healthy volunteers) and simple non-enzymatic ester cleavage to pharmacologically inactive products.
Olodaterol: In subjects with mild and moderate hepatic impairment systemic exposure to olodaterol was not affected. The effect of severe hepatic impairment on systemic exposure to olodaterol was not investigated.
Drug-Drug Interactions: Pharmacokinetic drug interaction studies with SPIOLTO RESPIMAT have not been performed; however such studies have been conducted with individual components tiotropium and olodaterol.
When tiotropium and olodaterol were administered in combination by the inhaled route, the pharmacokinetic parameters for each component were similar to those observed when each active substance was administered separately.
Tiotropium: An interaction study with tiotropium (14.4 mcg intravenous infusion over 15 minutes) and cimetidine 400 mg three times daily or ranitidine 300 mg once-daily was conducted. Concomitant administration of cimetidine with tiotropium resulted in a 20% increase in the AUC0-4h, a 28% decrease in the renal clearance of tiotropium and no significant change in the Cmax and amount excreted in urine over 96 hours. Co-administration of tiotropium with ranitidine did not affect the pharmacokinetics of tiotropium.
Common concomitant medications (long-acting beta2-adrenergic agonists (LABA), inhaled corticosterioids (ICS)) used by patients with COPD were not found to alter the exposure to tiotropium.
Olodaterol: Drug-drug interaction studies were carried out using fluconazole as model inhibitor of CYP 2C9 and ketoconazole as potent P-gp and CYP inhibitor.
Fluconazole: Co-administration of 400 mg fluconazole once daily for 14 days had no relevant effect on systemic exposure to olodaterol.
Ketoconazole: Co-administration of 400 mg ketoconazole once daily for 14 days increased olodaterol Cmax by 66% and AUC0-1 by 68%.
Tiotropium: Co-administration of tiotropium bromide, delivered as a fixed-dose combination with olodaterol, for 21 days had no relevant effect on systemic exposure to olodaterol, and vice versa.
Toxicology: Tiotropium + Olodaterol: Single-dose toxicity: For the combination tiotropium + olodaterol single-dose toxicity studies after inhalation administration have been performed for three dose ratios in mice and rats, revealing a low acute toxicity. In mice, the approximate lethal doses (ALD) were 34.8+36.6 mg/kg for tiotropium+olodaterol in the ratio 1:1. In rats, no deaths occurred, therefore the ALDs were >17.9+18.8 mg/kg for tiotropium/olodaterol in the ratio 1:1.
Repeat-dose toxicity: Inhalation repeat-dose toxicity studies for the combination tiotropium+olodaterol were performed in rats (4 weeks) and dogs (up to 13 weeks) at different dose ratios. In the 13-week studies in dogs, body weight development, clinical signs, changes of the cardiovascular system and of respective enzyme activities as well as the macroscopical and microscopical pathology were characteristic β2-agonistic and anticholinergic effects. In the 13-week toxicity studies with the dose ratio 1:1 for tiotropium/olodaterol, the no observed adverse effect levels (noael) were 14+16 microgram/kg/day.
Reproduction toxicity: No reproduction toxicity studies for the combination were performed.
Tiotropium: In the reproduction studies in rabbits and rats harmful effects with respect to pregnancy, embryo/fetal development, parturition or postnatal development could only be demonstrated at maternally toxic dose levels. In a general reproduction and fertility study in rats, there was no indication of any adverse effect on fertility or mating performance of either treated parents or their offspring at any dosage.
Olodaterol: In rats, no teratogenic effects occurred after inhalation at doses 1054 microgram/kg/day (>2600 times the human exposure (AUC(0-24h)) at the dose of 5 microgram). In pregnant NZW rabbits, an inhalation dose of 2489 microgram/kg/day (approximately 7130 times the human exposure at 5 microgram based on AUC(0-24h)) of olodaterol exhibited fetal toxicity characteristically resulting from β-adrenoceptor stimulation; these included patchy ossifications, short/bent bones, partially open eye, cleft palate, cardiovascular abnormalities. No significant effects occurred at a dose of 974 microgram/kg (approximately 1353 times the 5 microgram dose based on AUC(0-24h)). No impairment of male or female fertility or early embryonic development was seen in the rat up to inhalation doses of 3068 microgram/kg (approximately 2332 times the 5 microgram dose based on AUC(0-24h)).
No effects were observed on mating, fertility or bearing of live implants to Day 14/15/16 of gestation in the F1 animals in the rat up to inhalation doses of 3665 microgram/kg/day (approximately 2332 times the 5 microgram dose based on AUC(0-24h)).
Genotoxicity: In vitro mutagenicity for tiotropium or olodaterol alone, did not show any genotoxic potential. In the in vivo rat bone marrow micronucleus assay, after inhalation at dose levels of up to 2266+2174 microgram/kg/day tiotropium+olodaterol for 4 weeks (dose ratio 1:1), the combination was free of genotoxic potential.
In the in vivo rat bone marrow micronucleus assay after inhalation exposure (up to approximately 1092 times the 5 microgram dose based on AUC(0-24h)) and the in vitro (Ames test, mouse lymphoma assay) mutagenicity assays, olodaterol was free of any genotoxic potential up to very high dose levels. An increased frequency of micronuclei was observed in rats after i.v. exposure at doses of at least 5500-times the 5 microgram dose based on AUC(0-24h) may be related to drug enhanced (compensatory) erythropoiesis.
Carcinogenicity: No carcinogenicity studies for the combination were performed.
Tiotropium: Tiotropium did not show any carcinogenic potential in the respective studies in mice and rats.
Olodaterol: Lifetime treatment of rats induced class- and rodent-specific leiomyomas of the mesovarium at exposures approximately 2235-fold and 715-fold the exposure at the dose of 5 microgram dose (on systemic exposure). Lifetime treatment of mice induced class- and rodent-specific smooth muscle tumours (leiomyomas, leiomyosarcomas) of the uterus and incidences of sex cord stromal focal hyperplasia and luteal focal hyperplasia in the ovary at exposures approximately 477- to 3596-fold the exposure at the dose of 5 microgram dose (on systemic exposure), again considered as class- and rodent specific (exposure multiples). Both studies revealed no evidence for an olodaterol-related human risk with regard to carcinogenicity or chronic toxicity.